Hospital Equipment & Services by Auxo Medical
Running a hospital smoothly requires reliable medical equipment and expert support. At Auxo Medical, we’re dedicated to providing both. We offer a wide selection of new and refurbished medical equipment, comprehensive maintenance, and rapid repair services – all designed to keep your facility operating at peak efficiency.
Quality and Reliability: Our Foundation
We source equipment from top brands, ensuring performance and longevity. Our refurbished equipment undergoes rigorous quality checks, offering a cost-effective solution without sacrificing quality. We also supply brand-new equipment, giving you access to the latest technology for optimal patient care. Our commitment extends beyond sales; our highly trained technicians provide exceptional maintenance and repair services.
Comprehensive Equipment Solutions for Your Hospital
We offer a diverse range of equipment for various hospital departments:
Anesthesia Equipment: Ensuring Safe Procedures
We supply anesthesia machines, monitors, and booms from leading brands like Mindray and GE Healthcare. This includes:
- Anesthesia Machines: Reliable machines for various surgical settings. Regular maintenance ensures optimal performance.
- Anesthesia Monitors: Precise monitoring of vital signs during anesthesia, providing critical real-time data.
- Anesthesia Booms: Organized systems for delivering gases and utilities, enhancing efficiency and safety.
Biomedical Equipment: Supporting Patient Care
Our biomedical equipment selection includes:
- Patient Monitors: Accurate monitoring of vital signs, with various models to suit your needs.
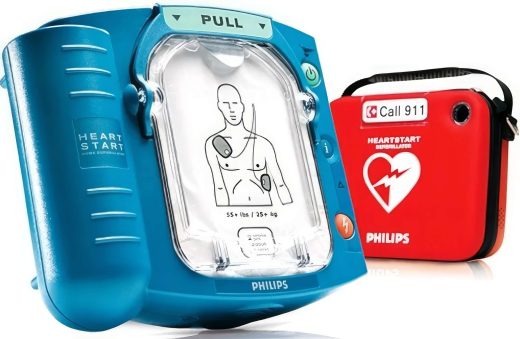
- Defibrillators: Life-saving devices, regularly inspected and maintained for immediate readiness.
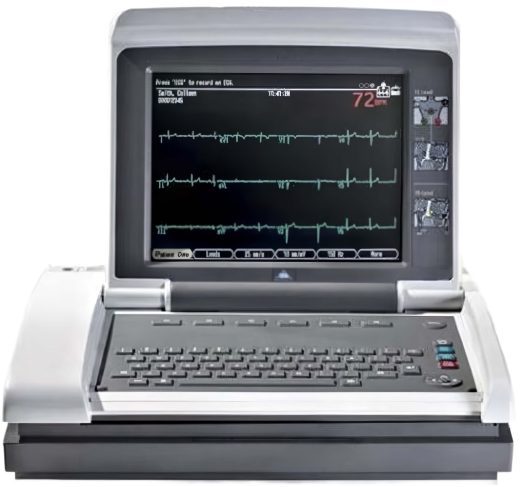
- ECG Machines: For recording and analyzing heart activity.
- Surgical Tables: Ergonomic tables designed for patient comfort and surgeon access.
- Exam Tables & Chairs: Comfortable and functional for patient examinations.
- Ventilators: Supporting respiratory function, with regular maintenance for optimal performance.
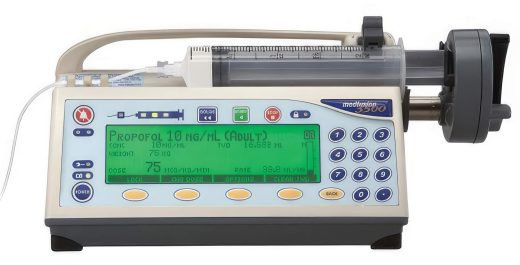
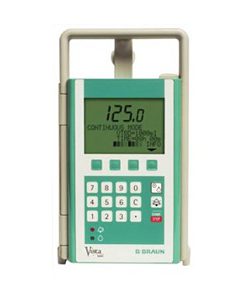
- Infusion & Syringe Pumps: Precise fluid delivery for various procedures.
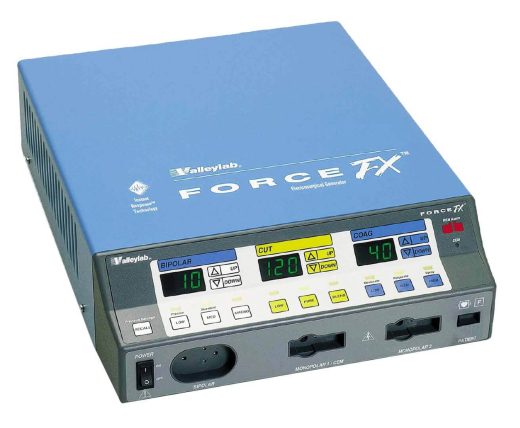
- Electrosurgical Units: For cutting and coagulating tissue during surgery, maintained for safety and effectiveness.
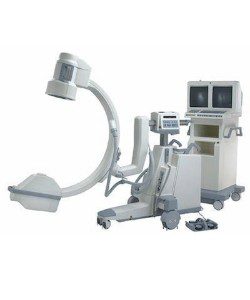
Imaging Equipment: Clearer Diagnostics
Advanced imaging is crucial for accurate diagnosis. We offer:
- C-Arms: Portable fluoroscopy systems for real-time imaging during surgery.
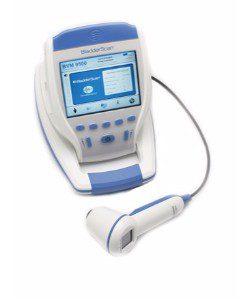
- Ultrasound Machines: For various diagnostic imaging applications, maintained for optimal image clarity.
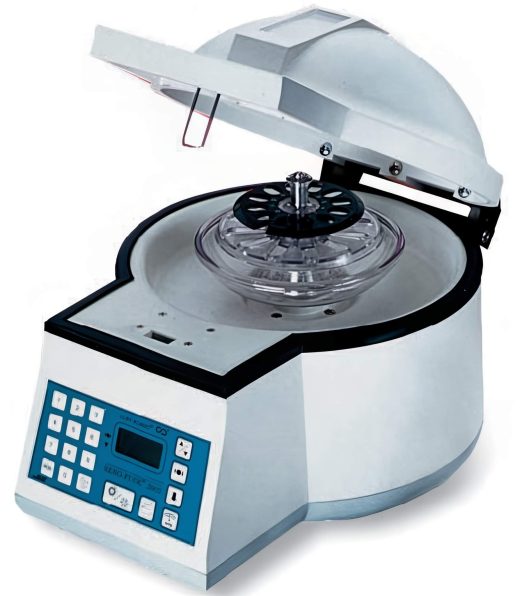
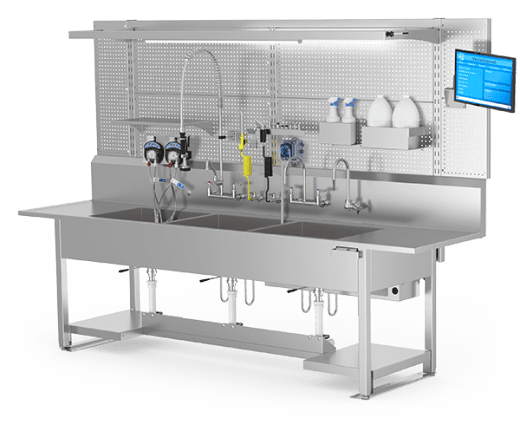
Sterile Processing Equipment: Maintaining a Sterile Environment
Maintaining sterility is paramount. Our equipment includes:
- Autoclaves: For sterilizing instruments and equipment using high-pressure steam.
- Sterilizers: Various sterilization methods to ensure optimal cleanliness.
- Washer-Disinfectors: For cleaning and disinfecting instruments before sterilization.
- Ultrasonic Cleaners: For thorough cleaning of delicate instruments.
- Boilers & Steam Generators: Providing steam for autoclaves and other sterilization equipment.
- Sterile Processing Supplies: Supporting your sterile processing operations.
Other Essential Equipment
We also offer:
- Hospital Beds: Comfortable and functional beds for patient care.
- Stretchers: For safe and efficient patient transport.
- Wheelchairs: Providing mobility solutions.
- Refrigerators/Freezers: For safe storage of medications and other temperature-sensitive items.
- Surgical Lighting: Optimal lighting for surgical procedures.
- Surgical Power Equipment: Power-driven instruments for surgical procedures.
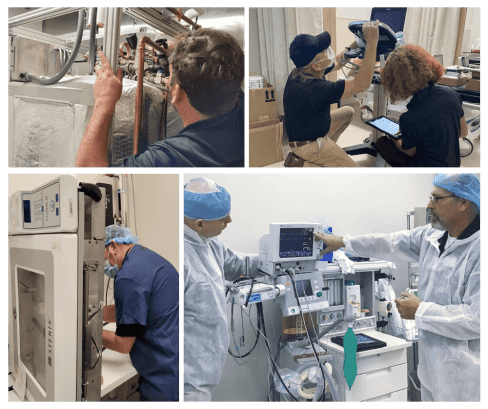
Expert Maintenance & Repair Services: Keeping Your Equipment Running
We’re committed to keeping your equipment running smoothly. Our team of highly skilled and trained technicians and engineers provide:
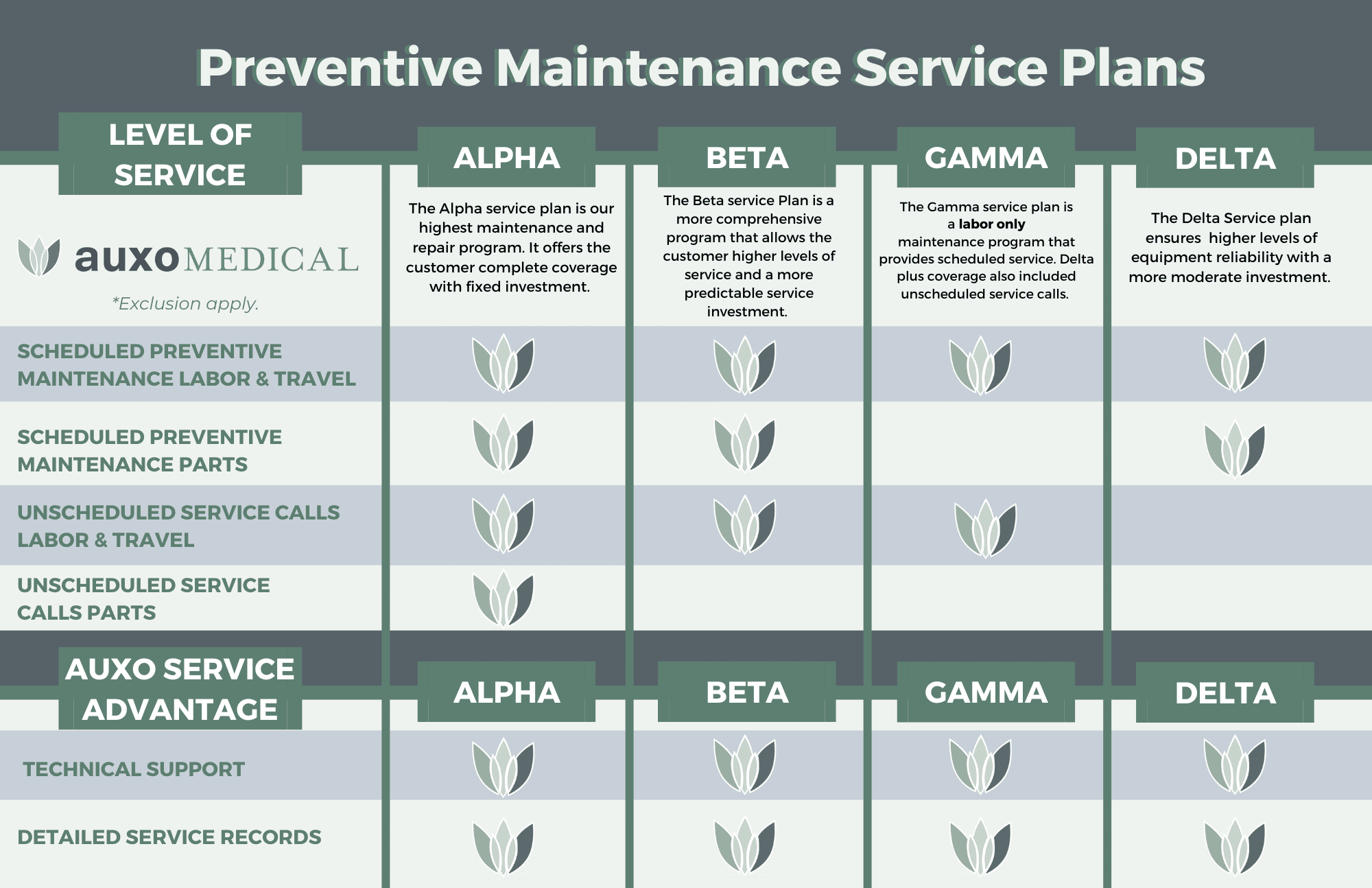
- Preventative Maintenance: Regular inspections and maintenance to prevent problems and extend equipment life. We offer tailored maintenance plans.
- Repairs: Fast, efficient repairs to minimize downtime.
- Inspections: Thorough checks to identify potential issues early.
- Calibrations: Ensuring accuracy and reliability.
- Parts Supply: A wide range of genuine and compatible parts.
- Equipment Upgrades & Refurbishment: Extending the life and improving the performance of your existing equipment.
Our Field Maintenance and Repair Service Areas
We provide comprehensive service and maintenance across numerous areas, including:
- Atlanta, GA
- Central Florida
- South Florida
- Dayton, OH
- Grand Rapids, MI
- Eastern Tennessee
- Lexington, KY
- Mid-Atlantic (VA, MD, NC, DC)
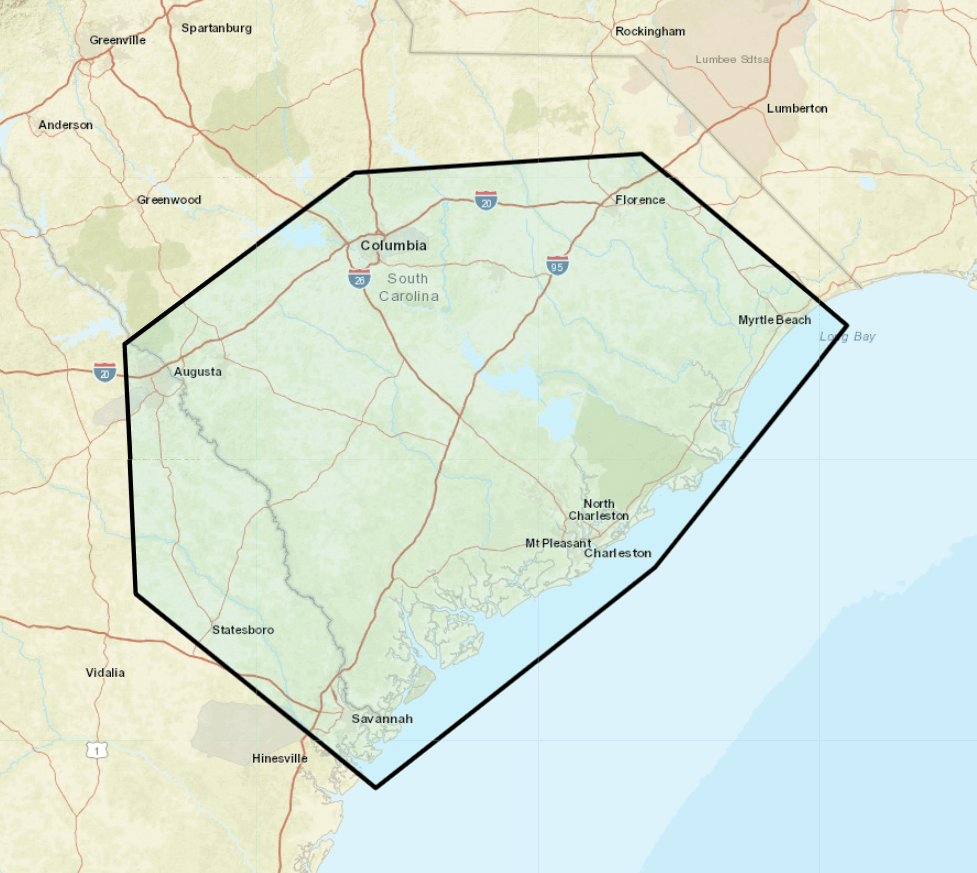
- South Carolina (Coming Soon)
Why Choose Auxo Medical?
- Expertise: Highly trained and experienced technicians.
- Comprehensive Services: From sales to maintenance and repairs.
- Cost-Effectiveness: Competitive pricing and cost-effective solutions.
- Reliability: Efficient service to minimize downtime.
- Customer Focus: Building strong, long-term relationships.
Auxo Medical is more than just a supplier; we’re your partner in ensuring your hospital operates efficiently and reliably. Contact us today to discuss your equipment needs. Call our office at (888) 728-8448.