Selecting the Right Autoclave for Healthcare Sterilization Needs
Effective sterilization is essential for safe healthcare delivery. Medical facilities need sterile surgical instruments, implants, gowns, and supplies to prevent transmitting infections. Autoclaves provide fast, reliable sterilization using steam under pressure to kill microbes on contaminated equipment. With a variety of models meeting different needs, selecting the right autoclave is key for optimal performance.
The Importance of Medical Sterilization
Reusing medical supplies without sterilization spreads dangerous pathogens like hepatitis, HIV, and Human Papilloma Virus (HPV). Proper sterilization eliminates over 99.9999% of microbes to prevent transmitting diseases through contaminated tools and devices.
Autoclaves are the workhorses delivering sterilization. Steam under high temperature and pressure penetrates wrapped instrument trays and devices to kill viruses, bacteria, and fungi. Effective sterilizers let clinical staff reuse tools safely while ensuring quality care.
Facilities like hospitals, clinics, dental offices, and surgery centers must invest in reliable, efficient autoclaves sized for their sterilization workloads. Units lasting 20+ years provide excellent longevity but require careful selection upfront.
Key Autoclave Considerations
With countless options available, choosing the right autoclave involves assessing several factors:
Needed Capacity – Larger facilities need high-volume autoclaves while small offices may only require tabletop models. Evaluate average instrument sets processed to determine ideal chamber size and cycle capacity.
Planned Utilization – Will the autoclave run all day or just a few cycles daily? Opt for larger units if consolidating sterilizers from multiple departments.
Available Space – Make sure allotted space matches the autoclave’s footprint requirements. Small offices have space constraints.
Types of Instruments – Certain devices like rigid endoscopes require special cycles. Verify the autoclave can process all planned instrument types.
Desired Cycle Types – Gravity vs. vacuum autoclaves offer different cycle options. Vacuum units are faster but more complex. Assess needed cycles.
Available Utilities – Ensure sufficient electrical supply, water access, and drainage exist at the autoclave location.
Budget – Hospital autoclaves carry higher price tags than office models. Consider total costs including installation and regular maintenance.
Taking time upfront to evaluate key requirements and facility constraints helps narrow the selections to models that best fit.
Autoclave Types by Size and Function
Autoclaves come in a variety of form factors each ideal for different use cases:
Countertop Autoclaves
Compact tabletop units with small chambers can process a few instrument sets per cycle. Their limited capacity suits small dental or medical offices. These are the most affordable options. Popular tabletop autoclave models include:
-
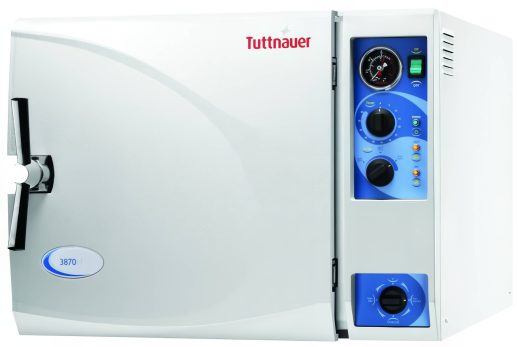
Tuttnauer 3870EA – 16 to 20 liter chamber
-
Statim 2000 – 2 liter fully self-contained cassette system
-
SciCan Bravo – 17 liter chamber size
Office Autoclaves
Slightly larger floor-standing units offer increased cycle capacity for small to mid-size facilities. Veterinary and dental offices often use these ~20 liter chamber models:
-
Tuttnauer 2340M – 23 liter chamber
-
Pelton Crane Validator 10 – 27 liter chamber
-
SciCan Elite – 22 liter chamber size
Hospital Autoclaves
Large-format autoclaves have spacious 40 liter+ chambers able to process full carts of instruments simultaneously. High loads suit central sterilization departments and sterile processing:
-
Tuttnauer 3870EL – 38 liter chamber
-
Steris Amsco Century – 40 liter chamber
-
Pelton Crane Magnaclave – 54 liter chamber
Waste Treatment Autoclaves
These heavy duty industrial autoclaves sterilize regulated medical waste and contaminated waste like gowns and linens prior to disposal. Chambers may exceed 130 liters.
-
Tuttnauer 2540EL – 164 liter chamber
Matching autoclave size to facility volumes prevents issues with under or overcapacity.
Choosing Between Gravity and Vacuum Autoclaves
Autoclaves utilize either gravity or vacuum technology for the steam exposure process:
Gravity Autoclaves
In gravity units, steam enters just from the top relying on gravity dispersion into the loads. Simple construction makes these very dependable but cycle times are slower ensuring steam penetration. Most smaller tabletop autoclaves use only gravity.
Vacuum Autoclaves
These autoclaves use vacuum pumps to first remove all the air from the chamber and instrument load. Steam is injected under pressure to penetrate loads rapidly and deeply. Cycles are much faster as steam infuses through the vacuums. Vacuum units need more maintenance.
Vacuum autoclaves provide faster cycles and better steam penetration but have higher upfront and maintenance costs. Evaluate tradeoffs based on workflow needs and device turnover requirements.
Special Cycles and Options
Modern autoclaves offer programmable cycles customized for different instruments and loads:
-
Wrapped Instruments – For wrapped surgical tool trays and medical devices.
-
Porosite/Textiles – Optimized for thick, porous loads like fabrics and linens.
-
Unwrapped Instruments – Fast exposed instrument cycles without wrapping.
-
Handpieces – Special cycles for sterilizing dental handpieces.
-
Empty Chamber – Heat and prep cycle to warm a cold autoclave.
-
Liquid – For directly sterilizing clean liquids in open containers.
-
Rectal probes – Unique cycles meeting longer exposure times.
Special options like vacuum drying, printer-recorders, doors that remain closed for drying, and double walls for cool outer surfaces may be available on some models. Accessory cages allow processing small loose items. Determine must-have cycle programs and options before purchasing.
Key Autoclave Brands
Reputable autoclave manufacturers include:
-
Tuttnauer – Full range of office and hospital autoclaves with many options. Excellent for high loads.
-
Steris – Reliable for sterile processing departments and waste treatment. Wide chamber capacity range.
-
Getinge – Vacuum autoclaves well suited for high turnover departments. Fast cycles.
-
Belimed – User-friendly designs for central sterile departments. Closed-door drying ability.
-
Midmark / Pelton Crane – Popular for dental offices. Compact all-in-one units.
-
SciCan – Intuitive autoclaves designed for dental and office use. Economical options.
Sticking with proven brands ensures acquiring a quality steam sterilizer backed by long-term OEM support and parts availability. Beware generic autoclave knockoffs which lack critical safety validation.
Maintaining Peak Autoclave Performance
Like any equipment, autoclaves need careful maintenance for continued peak operation:
-
Annual maintenance and calibration to meet healthcare standards
-
Regular recording printer paper replacement as directed
-
Monthly water reservoir draining and wiping
-
Proactive gasket, filter, and lamp replacement
-
Immediate repair of any fault indications or alarms
-
Validation testing per facility policies
Partnering with third-party service companies like Auxo Medical provides convenient upkeep to extend autoclave lifespans. Their expertise maintains sterilization capacity and regulatory compliance.
Acquiring Reliable Autoclaves
The right autoclave allows medical facilities to reuse instruments and devices safely. With such a significant investment, take time evaluating capacity requirements, cycles needed, and facility constraints before selecting a model. Reputable brands and regular preventative maintenance will pay dividends with years of sterilization capacity. Auxo Medical provides all major autoclave brands along with flexible purchasing options to meet diverse needs and budgets.
-
SteriData Logger Paperless Sterilizer Cycle Printer For Statim
$1,075.00 SteriData™ Logger for SciCan Statim 2000 and 5000 cassette sterilizers* (must have must have serial port in back and current software) The paperless alternative to a paper Printer This SteriData Logger unit plugs in just like the paper printer and… -
SteriData Logger Sterilizer Printer, Autoclave Printer, Paperless – Ritter / Midmark M9 / M11 Gen1 Series
$1,095.00 SteriData™ Logger for Midmark Ritter M9 and M11 Ultraclaves, M3 Ultrafast sterilizer, and SciCan Statim 2000 and 5000 cassette sterilizers* The paperless alternative to a paper Printer This SteriData Logger unit plugs in just like the paper printer and sits… -
Tuttnauer T-TOP 11B SFPP Autoclave
The Tuttnauer T-TOP 11B SFPP Autoclave offers advanced, reliable sterilization with user-friendly features designed to enhance efficiency in healthcare settings. This Class B pre/post vacuum autoclave utilizes steam flush pressure pulse (SFPP) technology, ensuring thorough sterilization without liquids, with programs… -
Alternative Data Logger to Midmark 9A682001 for M9/M11-040 through – 042
$795.00 The Autoclave Data Logger M42 is an alternative to the Midmark 9A682001 for third-generation Midmark M9 and M11 sterilizers with LCD displays and gray-white covers, specifically models ending with -040 through -042. Measuring approximately 2-1/2" x 4" x 1", this… -
Alternative Data Logger to Midmark 9A682001 for M9/M11-020 through – 022
$795.00 The Autoclave Data Logger M22 is a reliable alternative to the Midmark 9A682001 data logger for Midmark M9 and M11 sterilizers numbered -020 through -022. Sized at approximately 2-1/2" x 4" x 1", this wireless device includes a removable 16GB… -
Alternative Data Logger to Midmark 9A682001 for M9/M11-001 through – 019
$795.00 The Autoclave Data Logger M19 serves as an effective alternative to the Midmark 9A682001 data logger for older-style Midmark M9 and M11 sterilizers ending with -001 through -019. Designed for compatibility with Generation 1 Midmark autoclaves featuring a red display,… -
Steris AMSCO Century SG-160 Scientific Steam Sterilizer
The Steris AMSCO Century SG-160 Scientific Steam Sterilizer is a large-capacity, gravity-based sterilizer designed for rapid, reliable sterilization of heat- and moisture-stable materials. Featuring a spacious 26" x 37.5" x 60" (960 liters) chamber, it provides ample room to sterilize… -
Steris AMSCO Century SV-160 Scientific Steam Sterilizer
The Steris AMSCO Century SV-160 Scientific Steam Sterilizer is a high-capacity, pre-vacuum sterilizer engineered for rapid, dependable sterilization of heat- and moisture-stable materials. Featuring a generous chamber size of 26" x 37.5" x 60" (960 Liters), it accommodates large loads… -
Steris AMSCO Century SG-148 Scientific Steam Sterilizer
The Steris AMSCO Century SG-148 Scientific Steam Sterilizer is a high-capacity, gravity-based sterilizer designed for swift, reliable processing of heat- and moisture-stable materials. Featuring a spacious 26" x 37.5" x 48" (767 liters) chamber, it provides ample room to sterilize… -
Steris AMSCO Century SV-148 Scientific Steam Sterilizer
The Steris AMSCO Century SV-148 Scientific Steam Sterilizer is a high-capacity, pre-vacuum sterilizer engineered for rapid and reliable sterilization of heat- and moisture-stable materials. Boasting a spacious 26" x 37.5" x 48" (767 liters) chamber, it accommodates large loads of… -
Steris AMSCO SG-136 Scientific Medium Steam Sterilizer
The Steris AMSCO SG-136 Scientific Gravity Steam Sterilizer is a robust and efficient sterilization solution designed for reliable processing of heat- and moisture-stable materials. Featuring a spacious 26" x 37.5" x 36" (575 liters) chamber, it provides ample capacity to… -
Steris AMSCO SV-136 Scientific Medium Steam Sterilizer
The Steris AMSCO SV-136 Scientific Medium Steam Sterilizer is a high-capacity, pre-vacuum sterilizer designed for fast, reliable sterilization of heat- and moisture-stable materials. Featuring a spacious 26" x 37.5" x 36" (575 liters) chamber, it provides ample room to sterilize… -
Steris AMSCO Century Small Sterilizer – Steris SV-120 Steam Sterilizer
The Steris AMSCO SV-120 Small Steam Sterilizer is a high-performance, pre-vacuum sterilizer designed for reliable sterilization of nonporous, heat- and moisture-stable materials. Featuring a spacious 20" x 20" x 38" (250 liters / 66 gallons) chamber made from durable 316L… -
Steris AMSCO Century Small Sterilizer – Steris G-120 Steam Sterilizer
The Steris AMSCO G-120 Small Steam Sterilizer (also known as the G-120 Steris Sterilizer) is a high-quality, gravity-displacement steam sterilizer designed for reliable sterilization of nonporous, heat- and moisture-stable materials. Featuring a spacious 20" x 20" x 38" (250 liters… -
Steris AMSCO SV-116 Scientific Steam Sterilizer
The Steris AMSCO SV-116 Scientific Steam Sterilizer is a high-performance, pre-vacuum sterilizer designed for reliable sterilization of nonporous, heat- and moisture-stable laboratory items. With a spacious 16" x 16" x 26" (109 liters) chamber, it accommodates a variety of laboratory… -
Steris AMSCO 630LS Medium Steam Sterilizer
The Steris AMSCO 630LS Medium Sterilizer is a versatile and energy-efficient steam sterilizer designed for scientific and healthcare applications. It offers a spacious chamber, ideal for larger loads, and supports a range of sterilization cycles including pre-vacuum, gravity, liquid, leak… -
Steris AMSCO 110LS 16” (110L) Lab Sterilizer
The Steris AMSCO 110LS Lab Sterilizer is a fully refurbished 16-inch steam sterilizer designed for reliable sterilization in laboratory and healthcare environments. It features an interior chamber measuring 16" x 16" x 26" (110 liters), equipped with a rack and… -
Steris AMSCO Stage 3 Series 16″ 3011 Sterilizer – 110 Liters
The Steris AMSCO Stage 3 Series 16" (Model 3011) Sterilizer is a thoroughly refurbished, high-reliability steam sterilizer ideal for healthcare facilities. Equipped with a Stage 3 controller and thermal printer, it provides precise cycle documentation and a user-friendly thermal display… -
Steris AMSCO SG-116 Scientific Steam Sterilizer
The Steris AMSCO SG-116 Scientific Steam Sterilizer is a gravity-based sterilizer designed for the rapid sterilization of nonporous, heat- and moisture-stable goods, liquids, and media in life sciences and research settings. It features a 16" x 16" x 26" (109… -
Steris AMSCO C Series 20″ Sterilizer
The Steris C Series 20" Sterilizer is a expertly refurbished small steam sterilizer, expertly refurbished to meet OEM standards and upgraded to comply with the latest AAMI requirements. Designed for quick and efficient sterilization of heat- and moisture-stable materials, it… -
Tuttnauer T-TOP 11S SFPP Autoclave
The Tuttnauer T-TOP 11S SFPP Autoclave—a compact, high-performance sterilizer designed to simplify and accelerate your daily workflow. Its user-friendly LCD color touchscreen and intuitive icons make programming and monitoring effortless, while a multistage steam flush (SFPP) ensures fast, liquid-free sterilization.… -
Tuttnauer 3870M Autoclave (New)
The Tuttnauer 3870M Manual Autoclave offers reliable, efficient sterilization with user-friendly features like automatic shut-off at the end of both sterilization and drying cycles. Crafted with a durable, electro-polished chamber and door for long-lasting performance, it includes a double safety… -
Stainless Steel Side Panels for 400 Series 36in
Stainless Steel Side Panels for the 400 Series 36-inch Sterilizer are designed to provide durable, corrosion-resistant enclosure enhancements that protect the unit while enhancing its clinical aesthetics. Constructed from high-quality stainless steel, these panels offer superior durability in demanding hospital… -
36 inch cart and Carriage for 400 Series Sterilizer
The 36-inch cart and carriage for the Steris 400 Series 36-inch Sterilizer provide a robust, purpose-built transportation solution that ensures secure, stable handling of the recessed sterilizer. Designed to match the system’s dimensions, the cart features reinforced framing, smooth-rolling casters,… -
Steris 400 Series 36” House Steam Sterilizer Recessed
The Steris 400 Series 36" House Steam Sterilizer is a recessed, high-volume sterilization solution designed for efficiency and reliability. Its interior chamber measures 26 x 37.5 x 36 inches, with a fast, low-effort hinged-door option that locks or unlocks in… -
Steris Amsco 600 26.5 x 26.5 x 39″ Sterilizer
The Steris Amsco 600 is a sterilizer designed for efficient, high-volume processing, featuring a chamber with a 26.5 x 26.5" cross-section and a depth of 39" (450L volume). It offers 32 user-programmable cycle options, including pre-vacuum and gravity cycles, suitable… -
Scican Statim 5000 G4 Cassette Autoclave (New)
The SciCan Statim 5000 G4 Cassette Autoclave delivers a fully automatic and exceptionally fast sterilization solution for today's demanding practices. This brand-new unit utilizes four single-touch programs to optimize instrument cleaning from start to finish. Boasting a larger cassette and… -
Midmark Ritter M9 UltraClave (Autoclave), M9 UltraClave
The Midmark Ritter M9 UltraClave is a user-friendly automatic sterilizer designed for simple and reliable operation. Its automated features streamline the sterilization process: simply load the instruments, select the desired cycle, and press start. The M9 automatically fills with the… -
Steris AMSCO 250LS 20” (250L) Lab Sterilizer
The Steris 250LS 20'' Lab Sterilizer is a state-of-the-art steam sterilizer that has been meticulously refurbished to ensure optimal performance. Designed with a spacious interior chamber measuring 20x20x38 inches, it accommodates a wide range of sterilization needs. This sterilizer features… -
Midmark Ritter M11 UltraClave Veterinary Autoclave, M11-033
The Midmark Ritter M11 UltraClave Veterinary Autoclave, including the refurbished model with an 11" x 18" chamber, is renowned for its remarkable sterilizing capacity, making it an ideal choice for veterinary practices that handle larger packs and instruments. This countertop… -
Midmark M9D Manual Door Dental Autoclave
The Midmark M9D Manual Door Dental Autoclave (Refurbished) is a reliable and efficient solution for dental instrument sterilization. Designed to ensure precision and safety, this autoclave features an intuitive start button that automatically fills the chamber with the correct amount… -
Tuttnuaer 2540EK Kwiklave Electronic Autoclave (Refurbished)
The Tuttnauer 2540EK Kwiklave Electronic Autoclave, available in a refurbished model, is a versatile and efficient sterilization device ideal for various medical and laboratory settings. It offers four distinct programs—Unwrapped, Wrapped, Liquids, and a Drying cycle—facilitating comprehensive sterilization processes. Its… -
Cassette for Scican Statim G4 5000 Autoclave (Refurbished)
The Cassette for Scican Statim G4 5000 is an essential accessory designed to enhance the efficiency of the Statim sterilization process. Engineered for optimal performance, this cassette accommodates a wide range of dental and surgical instruments, ensuring effective steam sterilization… -
Cassette for Scican Statim G4 5000 Autoclave (New)
The Cassette for Scican Statim G4 5000 is an essential accessory designed to enhance the efficiency of the Statim sterilization process. Engineered for optimal performance, this cassette accommodates a wide range of dental and surgical instruments, ensuring effective steam sterilization… -
Steri-Dent 200 Dry Heat Sterilizer
The Steri-Dent 200 Dry Heat Sterilizer stands out as an exceptional method for sterilizing sharp instruments, effectively killing bacteria without moisture and preserving the sharpness of the tools. This versatile equipment not only serves as an efficient sterilizer but also… -
Tuttnauer T-TOP 10S Gravity Autoclave
The Tuttnauer T-TOP 10S Gravity Autoclave represents a significant advancement in sterilization technology, specifically designed for small clinics, laboratories, and other healthcare facilities. This model, known for its robust reliability and user-friendly interface, utilizes gravity displacement technology to effectively remove… -
Tuttnauer LABSCI 85LV Vertical Autoclave
The Tuttnauer LabSci 85LV Vertical Lab Autoclave is a state-of-the-art steam sterilizer designed to meet the demanding needs of educational institutions and research facilities. With a generous 85-liter chamber volume, this top-loading autoclave maximizes the efficiency of sterilization processes by… -
Tuttnauer LABSCI 60LV Vertical Autoclave
The Tuttnauer LabSci 60LV Vertical Lab Autoclave represents a significant advancement in steam sterilization technology, particularly suited for educational institutions and research facilities. This top-loading autoclave, part of Tuttnauer’s T-Lab ECO line, is engineered for economic and efficient sterilization of… -
Tuttnauer LABSCI15L+ Benchtop Autoclave
The Tuttnauer LABSCI15L+ Benchtop Autoclave stands as a premier solution for modern laboratories requiring reliable and efficient sterilization. With a generous 85L (approximately 17 gallons) chamber volume, this autoclave is equipped to handle a variety of materials—from glassware and instruments… -
Tuttnauer LABSCI15L Benchtop Autoclave
The Tuttnauer LABSCI 15L autoclave represents a pinnacle of convenience and reliability for laboratory sterilization needs. Engineered to handle a broad array of materials – from liquids and media to instruments, glassware, clothing, and even waste – this versatile unit… -
Tuttnauer LABSCI11L Benchtop Autoclave
The Tuttnauer LABSCI 11L autoclave is an essential tool for laboratory environments, designed with versatility and convenience in mind. This innovative system effectively sterilizes everything required in a lab setting, including liquids, media, instruments, glassware, clothing, and even waste. Its… -
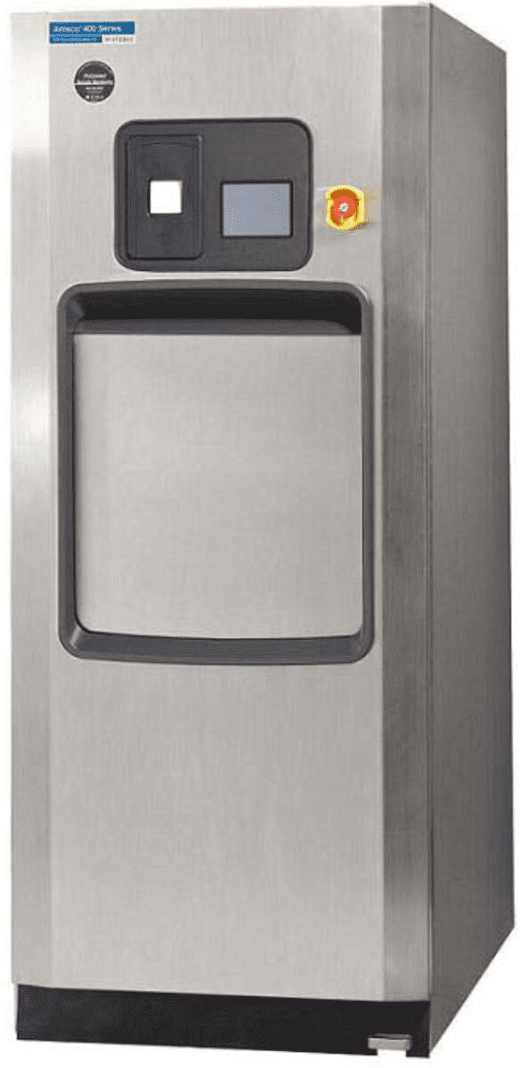
Steris Amsco 400 Series 48” House Steam Sterilizer Recessed
The Steris AMSCO 400 Series Medium Steam Sterilizer, with its 48-inch recessed design and spacious 26 x 37.5 x 48-inch chamber, is engineered for efficient, high-volume sterilization. The chamber's dimensions optimize loading capacity, allowing for effective processing of larger loads.… -
Tuttnauer DS1000 Steam Distiller 1 Gallon
The Tuttnauer DS1000 Steam Distiller 1Gal stands as a premier choice for those in need of high-quality, distilled water in laboratory, medical, or industrial settings. This compact yet powerful distillation unit is designed to convert tap water into pure, contaminant-free… -
Tuttnauer DS1G Steam Distiller 4L – 1L per Hr
The Tuttnauer DS1G Steam Distiller 4L represents a pinnacle of purification technology, specifically designed for those who demand the utmost in water purity. This compact, yet powerful device is capable of producing 4 liters of distilled water in just a… -
Tuttnauer 3870HSG-WS Pre/Post Vacuum 85L / 22.5 Gallon Autoclave
The Tuttnauer 3870HSG-WS autoclave is an 85 liter autoclave that is ideal for ASC’s and large clinics. The 3870HSG-WS autoclave provides hospital grade sterilization and medium loading capacity at a cost-effective price that meets the highest international standards. The… -
Tuttnauer Model 69B-SCP Pre-Vac Steam Sterilizer
The Tuttnauer Model 69B-SCP Pre-Vac Steam Sterilizer boasts an impressive array of features designed to meet the rigorous sterilization needs of modern laboratories and medical facilities. With its spacious internal chamber dimensions of 24"W x 36"H x 48"D, this free-standing… -
48inch cart and Carriage for 400 Series Sterilizer
The 48-inch cart and carriage system designed for the Steris 400 series 48-inch sterilizer exemplifies top-tier engineering and convenience in modern healthcare environments. Tailored to perfectly fit and enhance the functionality of the Steris 400 series 48-inch sterilizer, this cart… -
SteriData Logger Sterilizer Printer, Autoclave Printer, Paperless – Ritter / Midmark M9 / M11 NEW Series
$1,095.00 SteriData™ Logger for Midmark Ritter M9 and M11 Ultraclaves, M3 Ultrafast sterilizer, and SciCan Statim 2000 and 5000 cassette sterilizers* The paperless alternative to a paper Printer This SteriData Logger unit plugs in just like the paper printer and sits… -
Tuttnauer 3870E Autoclave
The refurbished Tuttnauer 3870E Autoclave offers a spacious 84-liter (22-gallon) capacity within its 15" x 27" chamber, accommodating substantial sterilization loads. Automated digital controls simplify operation, featuring a 60-minute timer and a clear digital display of temperature and pressure. The… -
Tuttnauer T-Edge 11S Gravity Autoclave
Fast Cycles: 36 Minute wrapped instruments complete cycle, including drying Optimal chamber capacity: More than 80% chamber capacity extra-long trays Convenient loading: Open to the door to 110º ensures it will not block your smooth loading of the chamber Remote… -
Tuttnauer T-Edge 11B Pre Post Vacuum Autoclave
Fast Cycles: 36 Minute wrapped instruments complete cycle, including drying Optimal chamber capacity: More than 80% chamber capacity extra-long trays Convenient loading: Open to the door to 110º ensures it will not block your smooth loading of the chamber Remote… -
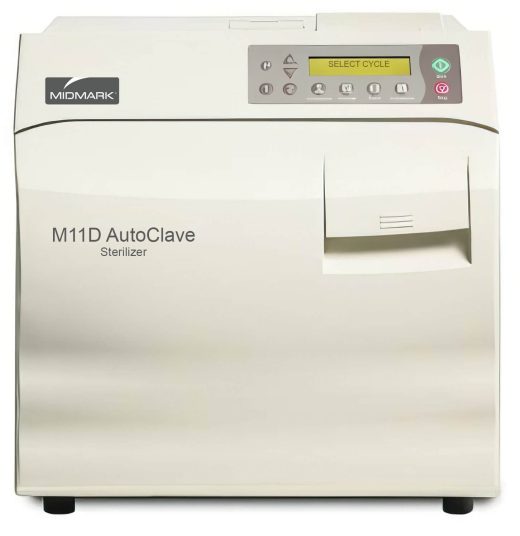
Midmark Ritter M11D Dental Manual Autoclave
The Midmark Ritter M11D Dental Manual Autoclave is a highly efficient and reliable sterilization solution, particularly noted for its refurbished model equipped with an expansive 11" x 18" chamber. This generous chamber size distinguishes it as the countertop sterilizer with… -
Tuttnauer Plazmax P50 Hydrogen Peroxide Sterilizer
The PlazMax sterilizer inactivates micro-organisms with Hydrogen Peroxide (H2O2) vapor and plasma. It sterilizes medical devices by diffusing H2O2 into the chamber and then converting the H2O2 molecules into a plasma state. The sterilization occurs inside the chamber by means… -
Tuttnauer EZ10k 220V Autoclave
The Tuttnauer EZ10k 220V Autoclave is a cutting-edge sterilization tool renowned for its efficiency and reliability in medical and laboratory settings. Designed with rapid cycle times, it features a fully automatic, user-friendly interface, making it ideal for high-demand environments where… -
Steris AMSCO LAB250 Steam Sterilizer
The Steris AMSCO LAB250 Steam Sterilizer is a compact, life-sciences oriented sterilizer designed for safe, reliable processing in research settings. It features a vertical sliding door with a non-lubricated steam-activated seal, a rugged vessel and reduced piping for dependability, and… -
Steris HC-900 Evolution Sterilizer
HC-900 26 x 37-1/2 x 42" Chamber AMSCO® Evolution® Steam Sterilizers are configured for prevacuum sterilization of heat- and moisture-stable materials used in healthcare facilities. These units can be equipped with prevacuum, Steam Flush Pressure Pulse (SFPP), gravity, liquid, and… -
Tuttnauer Plasmax 160 Hydrogen Peroxide Sterilizer
The PlazMax sterilizer inactivates micro-organisms with Hydrogen Peroxide (H2O2) vapor and plasma. It sterilizes medical devices by diffusing H2O2 into the chamber and then converting the H2O2 molecules into a plasma state. The sterilization occurs inside the chamber by means… -
Steris Amsco Stage 3 Series 20” 3023 Sterilizer
The refurbished Steris Amsco Stage 3 Series 20” 3023 Sterilizer offers a robust and reliable solution for demanding sterilization needs. Featuring a spacious 20" x 20" x 38" chamber and pre-vacuum (Class B) configuration, it ensures efficient and thorough sterilization… -
Steris AMSCO Stage 3 Series 16″ 3013 Sterilizer
The Steris AMSCO Stage 3 Series 16" (Model 3013) Sterilizer is a refurbished steam sterilizer designed for reliable sterilization in healthcare settings. It features a Stage 3 controller with an integrated thermal printer for accurate cycle documentation, and it is… -
Steris AMSCO Century Small Sterilizer – Steris V-120 Steam Sterilizer
The Steris AMSCO Century Small Sterilizer (Steris V-120 Steam Sterilizer), is an advanced solution tailored to meet the demands of today's operating rooms and various hospital environments. This sterilizer boasts a spacious chamber measuring 20" x 20" x 38", capable… -
Ritter M11 Autoclave, M11-001 – RENTAL
Refurbished Ritter M11 with 11" x 18" chamber. It's chamber size gives it the distinction of having the largest sterilizing capacity of any standard countertop sterilizer on the market, making it perfect for larger packs and instruments. [vc_btn title="Download Brochure"… -
Tuttnauer 2540M Autoclave
The Tuttnauer 2540M Autoclave is a reliable, cost-effective sterilization solution designed for daily use with minimal maintenance. Featuring an automatic shut-off at the end of both sterilization and dry cycles, a dual safety thermostat for overheating protection, and a durable… -
Steris Amsco 400 Series 20″ Sterilizer
The refurbished Steris Amsco 400 Series 20" steam sterilizer offers a reliable and efficient solution for sterilization needs. Its 20"x20"x38" chamber accommodates a rack and two-shelf loading system, maximizing throughput. The single, foot-pedal actuated vertical power door simplifies loading and… -
Steris Amsco Eagle 3053
Refurbished Steris Eagle 3053 Steam Sterilizer Refurbished Steris Amsco Eagle 3000 Stage 3 series, 24″x 36″ x 60″, single door sterilizer. Recess mounted, or optional cabinet package. Model 3053. Pre-vac sterilizer, (3051 variant for gravity operation) with operating temperature of… -
Steris Amsco Eagle 3043
Refurbished Steris Eagle 3043 Steam Sterilizer Refurbished Steris Amsco Eagle 3000 Stage 3 series, 24″x 36″ x 48″, single door sterilizer. Recess mounted, or optional cabinet package. Model 3043. Pre-vac sterilizer, (3041 variant for gravity operation) with operating temperature of… -
Steris Amsco Eagle 3033 Steam Sterilizer
The refurbished Steris Amsco Eagle 3033 Steam Sterilizer offers a large 24" x 36" x 36" chamber for high-volume sterilization needs. This recess-mountable unit (with optional cabinet package) features the advanced Stage 3 controller with a thermal printer for precise… -
Steris AMSCO Century V-160 (160H and G-160) Steam Sterilizer
he Steris AMSCO Century V-160 family (160H and G-160) is a fast, efficient pre-vacuum steam sterilizer designed for heat- and water-resistant loads. Featuring a 26" x 37.5" x 60" (960 Liters) chamber and pre-vacuum, gravity, flash, express, leak test, and… -
Steris AMSCO Century V-148 Steam Sterilizer (148H and G-148)
The Steris AMSCO Century V-148 Steam Sterilizer (148H and G-148) is a fast, efficient pre-vacuum steam sterilizer designed for heat- and water-resistant loads, delivering the same capabilities as a gravity model with enhanced processing speed. It features a 26" x… -
Steris AMSCO V-136 (136H and G-136) Steam Sterilizer
The Steris AMSCO V-136 Steam Sterilizer (136H and G-136) is a fast, efficient pre-vacuum sterilizer designed for heat- and water-resistant loads, delivering the performance of a gravity model with streamlined processing. Featuring a 26" x 37.5" x 36" (575 L)… -
Dri-Clave 3000 Dry Heat Sterilizer 3 Tray
The FDA approved technique of dry heat sterilization works without pressure, steam, or chemicals. Dry heat sterilizes in the shortest possible time and you never need to dry the instruments. Ideal for all medical and dental instruments, it sterilizes instruments,… -
Tuttnauer 3870M Autoclave (Refurbished)
The Tuttnauer 3870M Manual Autoclave stands as the largest manual table-top autoclave offered by Tuttnauer, continuing to fulfill a significant demand in healthcare facilities and veterinary practices. This robust, straightforward unit provides essential sterilization capabilities, proving reliable even in challenging… -
Scican Statim 5000 G4 Cassette Autoclave (Refurbished)
The SciCan Statim 5000 G4 Cassette Autoclave offers a fully automatic and exceptionally fast sterilization solution for busy practices. This refurbished unit utilizes four single-touch programs to optimize instrument cleaning from start to finish. With a larger cassette and an… -
Dri-Clave Dry Heat Sterilizer – 2 Tray
The FDA approved technique of dry heat sterilization works without pressure, steam, or chemicals. Dry heat sterilizes in the shortest possible time and you never need to dry the instruments. Ideal for all medical and dental instruments, it sterilizes instruments,… -
Pelton & Crane Validator 10
The Pelton & Crane Validator 10 Autoclave is a economical, light-capacity sterilizing unit designed to accommodate the needs of small medical, dental, and other practices requiring reliable and safe access to sterilization equipment. Incorporated are a variety of safety and… -
Midmark Ritter M11 Ultraclave (Autoclave), M11-022
The refurbished Midmark Ritter M11 Ultraclave (Autoclave) offers a compact yet spacious sterilization solution with its 11" x 18" chamber, touted as the largest among standard countertop sterilizers. This increased capacity makes it ideal for processing larger instrument packs and… -
Tuttnauer EZ10
The Tuttnauer EZ10 Fully Automatic Medical Autoclave Sterilizer features a simple one-touch design and pre-programmed cycles for: unwrapped instruments, wrapped and packs, glassware and an additional drying cycle. The Tuttnauer EZ10 Fully Automatic Autoclaves fill, sterilize, exhaust and dry at… -
Ritter M11 Autoclave, M11-001
Refurbished Ritter M11 with 11" x 18" chamber. It's chamber size gives it the distinction of having the largest sterilizing capacity of any standard countertop sterilizer on the market, making it perfect for larger packs and instruments. [vc_btn title="Download Brochure"… -
Tuttnauer 2340EA Autoclave
This table-top autoclave is designed for the sterilization of wrapped and unwrapped instruments, glassware and other related items found in dental, medical and veterinary clinics, tattoo parlors, first aid rooms, hospitals, laboratories and other related industries. [vc_btn title="Download Brochure" style="flat"…






























































































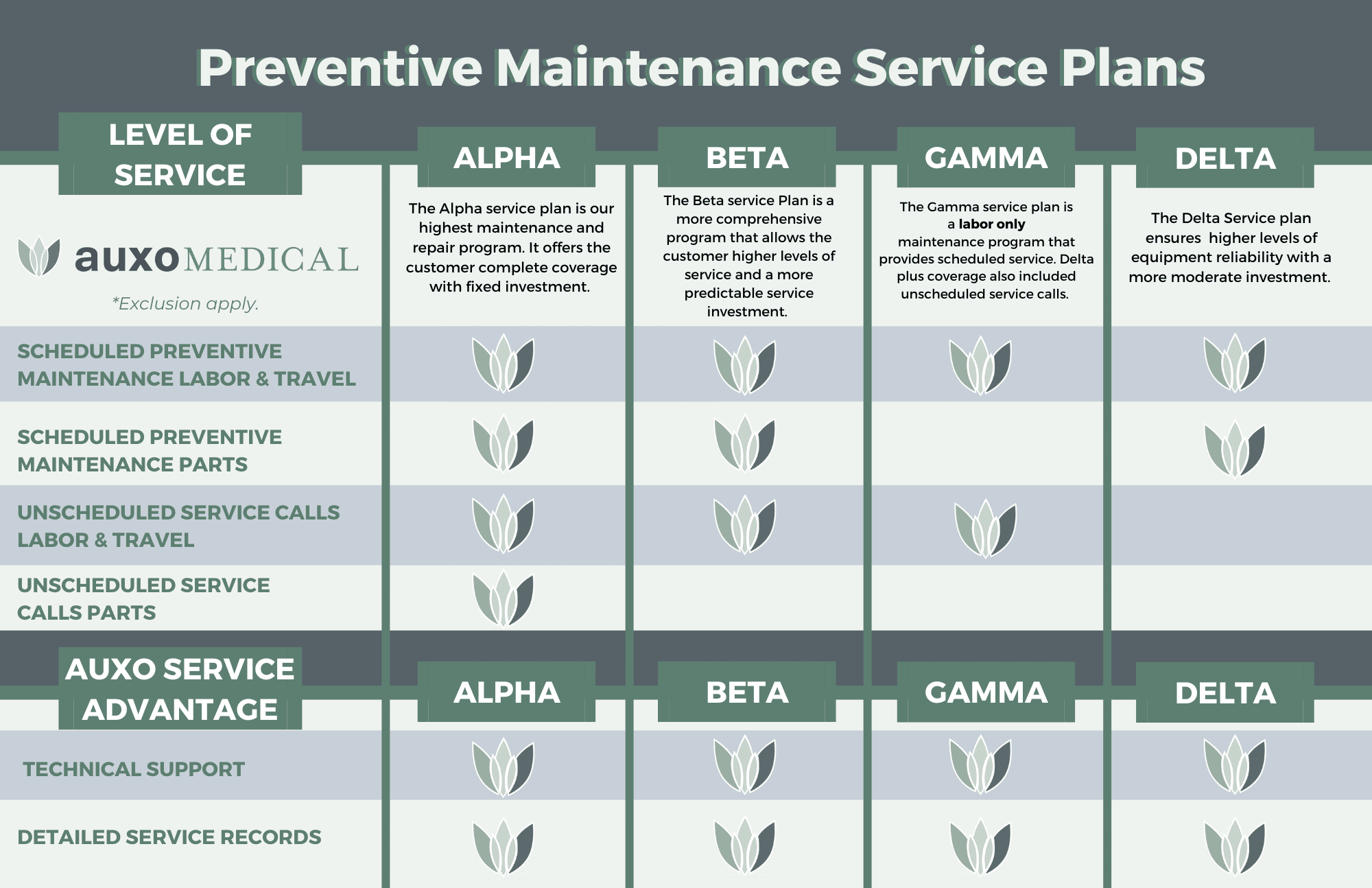 Preventative Maintenance (PM)
Preventative Maintenance (PM)

 One of the best ways to avoid costly downtime is through scheduled preventative maintenance. At Auxo Medical, we offer custom PM plans equivalent or superior to manufacturer programs, but at a lower hourly repair rate.
One of the best ways to avoid costly downtime is through scheduled preventative maintenance. At Auxo Medical, we offer custom PM plans equivalent or superior to manufacturer programs, but at a lower hourly repair rate.