Featured Electrosurgical and Smoke Evacuation Equipment
At Auxo Medical, we offer a comprehensive selection of high-quality electrosurgical and smoke evacuation equipment designed to enhance surgical precision, safety, and hygiene in your facility. Our product lineup includes industry-leading platforms, generators, and smoke evacuation systems from top brands like Covidien Valleylab, Medtronic Valleylab, ConMed, and Aaron Bovie, all backed by dedicated support and service.
Featured Electrosurgical Platforms and Generators
Covidien Valleylab Force Triad™
The Valleylab Force Triad™ energy platform is renowned for its versatility and advanced technology, providing surgeons with reliable RF energy delivery for a wide range of procedures. Request a quote today to upgrade your surgical capabilities.
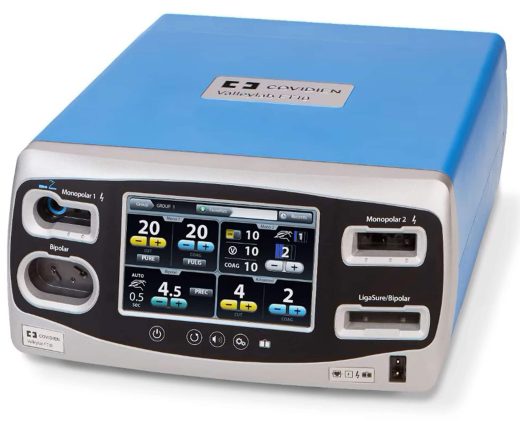
Medtronic Valleylab FT10 Energy Platform
Designed for precision and efficiency, the Valleylab FT10 offers advanced energy management for delicate and complex surgeries. Contact us for pricing and more details.
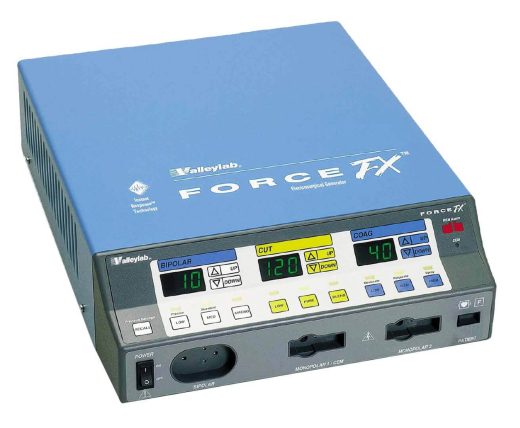
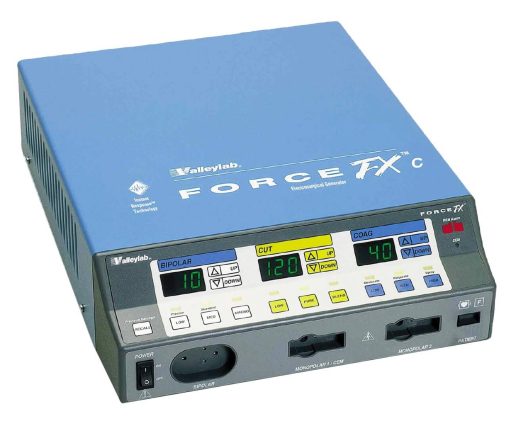
Valleylab Force FX™
The Valleylab Force FX™ generator combines power and safety features to deliver optimal RF energy during surgical procedures. Reach out to us for a quote and discover how it can benefit your practice.
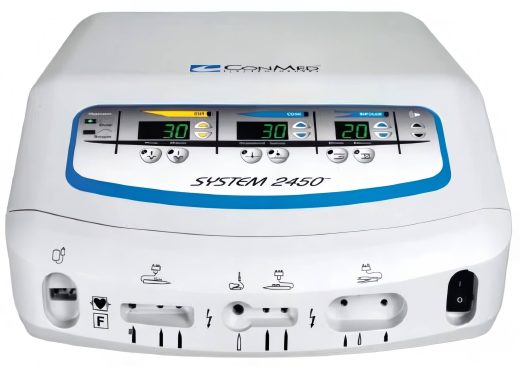
ConMed 2450 Electrosurgical Unit
Offering reliable performance, the ConMed 2450 Electrosurgical Unit is an excellent choice for various surgical applications. Request a quote to learn more.
Infinium Edge Series
The Infinium Edge 200 and Edge 400 Electrosurgery Units provide flexible and advanced energy solutions, supporting a wide range of surgical needs. Contact us for additional information and pricing.
Smoke Evacuation Systems
ConMed AER DEFENSE Smoke Evacuation System
Ensure a safer surgical environment with the ConMed AER DEFENSE Smoke Evacuation System. Designed for efficient smoke removal, it helps maintain clear visibility and reduce airborne contaminants. Request a quote today.
ValleyLab Force Optimumm Smoke Evacuator
The ValleyLab Force Optimumm Smoke Evacuator Unit offers powerful smoke evacuation with easy operation, helping to improve safety and compliance during procedures. Contact us for details.
Aaron Bovie Smoke Evacuators
- Aaron Bovie SE2 Smoke Shark Evacuator: Compact and powerful, ideal for a variety of surgical environments. Request a quote to upgrade your smoke management system.
- Aaron Bovie A2350 Bovie Surgi-Center | PRO: A 200W electrosurgical generator with advanced safety features, perfect for high-precision surgeries. Request a quote for this versatile system.
Why Choose Auxo Medical?
Auxo Medical provides top-tier electrosurgical and smoke evacuation equipment tailored to your clinical needs. Our team offers expert consultation, competitive pricing, and comprehensive support to ensure your facility operates at peak efficiency.
-
Aaron Bovie A2350 – Bovie Surgi-Center | PRO 200W Electrosurgical Generator
The Aaron Bovie A2350 Surgi-Center|PRO is a high-power, 200-watt electrosurgical generator designed for the operating room, offering advanced surgical precision with safety features at a significant cost savings. It provides 12 monopolar and bipolar RF energy modalities, including specialized modes… -
Aaron Bovie SE2 Smoke Shark Evacuator
The Aaron Bovie SE2 Smoke Shark Evacuator is an advanced, lightweight, and compact smoke evacuation system designed to efficiently remove smoke and particulates during surgical procedures. Its modern design makes it easy to use, store, and stack, optimizing space in… -
Conmed 2450 Electrosurgical Unit
The ConMed 2450 Electrosurgical Unit is a versatile electrosurgical generator designed for a range of surgical procedures. It features Dynamic Response technology, which synchronizes voltage and current to deliver optimal clinical effects across all modes. The unit has a maximum… -
ConMed AER DEFENSE Smoke Evacuation System
The ConMed AER DEFENSE Smoke Evacuation System is designed to remove surgical smoke, protecting staff and patients from its hazards. It features four operational modes for versatility and is notably quiet, operating 11% (7 dBA) quieter than previous models. The… -
Valleylab Force FX
The Valleylab Force FX™ generator offers surgeons precise power delivery, even through resistant tissue, thanks to its innovative Instant Response™ technology. This technology optimizes performance at lower power settings, reducing the risk of tissue damage, neuromuscular stimulation, and the need… -
Infinium Edge 400 Electrosurgical Generator
The Infinium EDGE 400 is a state-of-the-art high-frequency electrosurgical generator designed for both monopolar and bipolar surgical procedures, offering a broad spectrum of high-precision applications. Engineered for minimally invasive surgeries, it excels in resection, evaporation, and coagulation tasks. The system… -
Infinium Edge 200 Electrosurgery Unit
The Infinium EDGE 200 is a state-of-the-art high-frequency electrosurgical generator designed for both monopolar and bipolar surgical procedures, making it an ideal choice for surgery centers focused on minimally invasive techniques. Engineered to perform resection, evaporation, and coagulation, the EDGE… -
Medtronic Covidien Valleylab FT10 Energy Platform (VLFT10GEN)
$18,995.00 This professionally refurbished Medtronic Covidien Valleylab FT10 Energy Platform (OEM: VLFT10GEN) is a high-performance, multi-generator energy platform designed to power a full range of energy-based surgical devices, including monopolar, bipolar, and LigaSure vessel-sealing instruments. Key features include tissue impedance-based TissueFect… -
Covidien Valleylab Force Triad
The Covidien Valleylab Force Triad™ is a comprehensive energy platform that integrates electrosurgical cutting and coagulation, bipolar functionality, and advanced vessel sealing into a single generator. Featuring TissueFect™ sensing technology, this system precisely manages energy delivery for optimal results. The… -
ValleyLab Force Optimumm Smoke Evacuator Unit
The OptiMumm Smoke Evacuator is the centerpiece of a complete smoke evacuation system when used with the AccuVac Smoke Evacuation attachment, Valleylab's Universal Mounting System, and either the Force FX Electrosurgical Generator or the Force EZ Electrosurgical Generator. [vc_btn title="Download…